





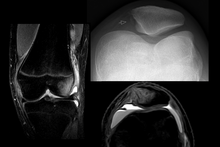
Radiograph of a patient with patellar dislocation. Normally the patella projects over the distal femur.
|
The patella generally dislocates laterally, and can be accompanied by acute pain and disability. Immediate reduction can be accomplished by hyperextension of the knee, and by providing a medialward pressure to move the patella back into the patellofemoral groove. Hyperextension of the knee on its own could possibly move the patella into place, because this motion locks the knee in place. When the knee is locked the ligaments are twisted and taut, allowing the muscles involved to relax and the patella to slide back into place. If that does not work, a medical professional must manually perform an orthopedic reduction. Swelling and impaired mobility follow patellar dislocation, and a rehabilitation program of six to sixteen weeks is recommended whether or not the patient undergoes surgery.
Young athletes suffer patellar dislocations more commonly than any other group, and the average age of occurrences is 16–20 years. Sports commonly associated with the injury involve sudden twisting motions of the knee and/or impact, such as soccer,gymnastics and ice hockey. It can also occur when a person trips over an object or slips on a slick surface, especially if that person has predisposing factors.
Top of page
Anatomy of the knee

The patella is a triangular sesamoid bone which is embedded in tendon. It rests in the patellofemoral groove, an articular cartilage-lined hollow at the end of the thigh bone (femur) where the thigh bone meets the shin bone (tibia). Several ligaments and tendons hold the patella in place and allow it to move up and down the patellofemoral groove when the leg bends. The top of the patella attaches to the quadriceps muscle via the quadriceps tendon, the middle to the vastus medialis obliquus and vastus lateralismuscles, and the bottom to the head of the tibia (tibial tuberosity) via the patellar tendon, which is a continuation of the quadriceps femoris tendon. The medial patellofemoral ligament attaches horizontally in the inner knee to the adductor magnus tendon and is the structure most often damaged during a patellar dislocation. Finally, the lateral collateral ligament and the medial collateral ligament stabilize the patella on either side. Any of these structures can sustain damage during a patellar dislocation.
Top of page
Mechanism of injury
Patellar dislocations occur by:
- A direct impact that knocks the patella out of joint
- A twisting motion of the knee, or ankle
- A sudden lateral cut
Top of page
Children
Lateral Patellar dislocation is common among the child population. Some studies suggest that the annual patellar dislocation rate in children is 43/100,000. The treatment of the skeletally immature is controversial due to the fact that they are so young and are still growing. Surgery is recommended by some experts in order to repair the medial structures early, while others recommend treating it non operatively with physical therapy. If re-dislocation occurs then reconstruction of the medial patellofemoral ligament (MPFL) is the recommended surgical option.
Top of page
Predisposing factors
Athletic Population
- Patellar dislocation occurs in sports that involve rotating the knee.
- Direct trauma to the knee can knock the patella out of joint.
Positive Family History[edit]
- 24% of patients whose patellas have dislocated have relatives who have experienced patellar dislocations.
Anatomical Factors
Excessive Q-angle
Misalignment of the patella on the knee joint
Insufficient Vastus Medialis Obliquus Muscle (VMO)
Top of page
Symptoms and signs
Patients often describe pain as being “inside the knee cap.” The leg tends to flex even when relaxed. In some cases, the injured ligaments involved in patellar dislocation do not allow the leg to flex almost at all.
To assess the knee, a clinician can perform the Patellar Apprehension Test by moving the patella back and forth while the patient flexes the knee at approximately 30 degrees.
The patient can do the patella tracking assessment by making a single leg squat and standing, or by lying on his or her back with knee extended from flexed position. A patella that slips medially on early flexion is called the J sign, and indicates imbalance between the VMO and lateral structures.
Forces
When there is too much tension on the patella, the ligaments will weaken and be susceptible to tearing ligaments or tendons due to shear force or torsion force, which then displaces the kneecap from its origination. Another cause that patellar dislocation can occur is when the trochlear groove that has been completely flattened is defined astrochlear dysplasia. Not having a groove because the trochlear bone has flattened out can cause the patella to slide because nothing is holding the patella in place.
Top of page
Treatment options
Two types of treatment options are typically available:
- Surgery
- Conservative treatment (rehabilitation and physical therapy)
Surgery may impede normal growth of structures in the knee, so doctors generally do not recommend knee operations for young people who are still growing. There are also risks of complications, such as an adverse reaction to anesthesia or an infection.
When designing a rehabilitation program, clinicians consider associated injuries such as chipped bones or soft tissue tears. Clinicians take into account the patient's age, activity level, and time needed to return to work and/or athletics. Doctors generally only recommend surgery when other structures in the knee have sustained severe damage, or specifically when there is:
- Concurrent osteochondral injury
- Continued gross instability
- Palpable disruption of the medial patellofemoral ligament and the vastus medialis obliquus
- High-level athletic demands coupled with mechanical risk factors and an initial injury mechanism not related to contact
Supplements like glucosamine and NSAIDs can be used to minimize bothersome symptoms.
Top of page
Post-treatment rehabilitation
An effective rehabilitation program reduces the chances of reinjury and of other knee-related problems such as patellofemoral pain syndrome and osteoarthritis. Rehabilitation focuses on maintaining strength and range of motion to reduce pain and maintain the health of the muscles and tissues around the knee joint.
Prevention
The patella is a floating sesamoid bone held in place by the quadriceps muscle tendon and patellar tendon ligament. Exercises should strengthen quadriceps muscles such asrectus femoris, vastus intermedius, and vastus lateralis. However, tight and strong lateral quadriceps can be an underlying cause of patellar dislocation. If this is the case, it is advisable to strengthen the medial quadriceps, vastus medialis (VMO), and stretch the lateral muscles. Exercises to strengthen quadriceps muscles include, but are not limited to, squats and lunges. Adding extra external support around the knee by using devices such as knee [orthotics] or athletic tape can help to prevent patellar dislocation and other knee-related injuries. External supports, such as knee braces and athletic tape, work by providing movement in only the desired planes and help hinder movements that can cause abnormal movement and injuries. Women who wear high heels tend to develop short calf muscles and tendons. Exercises to stretch and strengthen calf muscles are recommended on a daily basis.